


1Department of Dermatology, Tenon Hospital, Public Assistance – Paris Hospitals (AP-HP), Paris, 2Vascular Medicine Department, Grenoble University Hospital, Grenoble, 3Department of Public Health, Tenon Hospital, AP-HP, Pierre and Marie Curie University, and the French National Institute of Health and Medical Research, UMR-S 1136, Paris, 4Department of Dermatology and Photobiology, Nord Hospital, Grenoble University Hospital Centre, Grenoble, Departments of Dermatology: 5Brabois Hospital, Nancy University Hospital Centre, Nancy, 6Le Mans Hospital, Le Mans, 7Sainte-Anne Military Hospital, Toulon, 8Amiens University Hospital, Amiens, and 9Tenon Hospital, AP-HP, and Pierre and Marie Curie University, Paris, France
Lower-limb ulcers in systemic sclerosis patients are rarely reported. The aim of this study was to describe the main causes and outcomes of lower-limb ulcers in systemic sclerosis patients and to assess factors associated with ischaemic causes (arterial disease and/or microvascular impairment). A retrospective, multicentre, case-control study was conducted in 2013 and 2014, including 45 systemic sclerosis patients presenting lower-limb ulcers between 2008 and 2013. The estimated prevalence of lower-limb ulcers among systemic sclerosis patients was 12.8%. Ulcers were related to venous insufficiency in 22 cases (49%), ischaemic causes in 21 (47%) and other causes in 2 (4%). Complete healing was observed in 60% of cases in a mean time of 10.3 months; 59% relapsed during a mean follow-up of 22 months. Ischaemic lower-limb ulcer outcomes were poor, with a 28.6% amputation rate. Logistic-regression multivariate analyses between ischaemic lower-limb ulcer cases and matched systemic sclerosis-controls identified past or concomitant digital ulcer and cutaneous sclerosis of the feet as independent risk factors associated with ischaemic lower-limb ulcers.
Systemic sclerosis is a chronic connective tissue disorder responsible for skin fibrosis, in which skin ulcers are frequent and severely affect the patient’s quality of life. Nevertheless, only few series investigated lower limb ulcers in systemic sclerosis. This retrospective study describes lower limb ulcers clinical characteristics, causes and outcomes in patients with systemic sclerosis, highlighting the poor prognosis and the risk of amputation in case of ischaemic causes. Secondly, we performed analyses comparing subgroups (with or without lower limbs ulcers) of patients with systemic sclerosis to identify factors associated with their development during systemic sclerosis.
Key words: systemic sclerosis; lower-limb ulcers; ischaemic ulcers.
Accepted Apr 12, 2018; Epub ahead of print Apr 12, 2018
Acta Derm Venereol
Corr: Patricia Senet, MD, Department of Dermatology, Tenon Hospital, AP-HP,
4, rue de la Chine, FR-75020 Paris, France. E-mail: patricia.senet@aphp.fr
Systemic sclerosis (SSc) is a chronic connective tissue disorder characterized by immune-system activation, vascular involvement and fibroblast dysfunction leading to collagen accumulation responsible for skin fibrosis and internal organ involvement (1). Skin ulcers occur in 35% to 60% of SSc patients and severely affect patients’ quality of life and daily activities (2–4). Upper-limb ischaemic digital ulcers (DUs) secondary to microcirculation vasculopathy are the most common ulcers in SSc and are extensively described in cohorts (4–7). Few series have investigated SSc-associated lower-limb ulcers (LLUs) and little data on the causes of LLU and their outcomes in SSc patients is available (8–11), but some studies highlight the poor healing prognosis and the risk of amputation in case of ischaemic causes of LLU. We, therefore conducted a multicentre, retrospective study to describe the clinical characteristics, causes and outcomes of LLU in SSc patients and to identify factors associated with the development of ischaemic LLU during SSc.
This retrospective, case-control, multicentre study was conducted between December 2013 and July 2014. It was carried out in compliance with Good Clinical Practices and the Declaration of Helsinki, in accordance to French law. Formal approval by an ethics committee was not required in 2014 for this type of study (Articles L1121-1 and R1121-3 of the French Public Health Code).
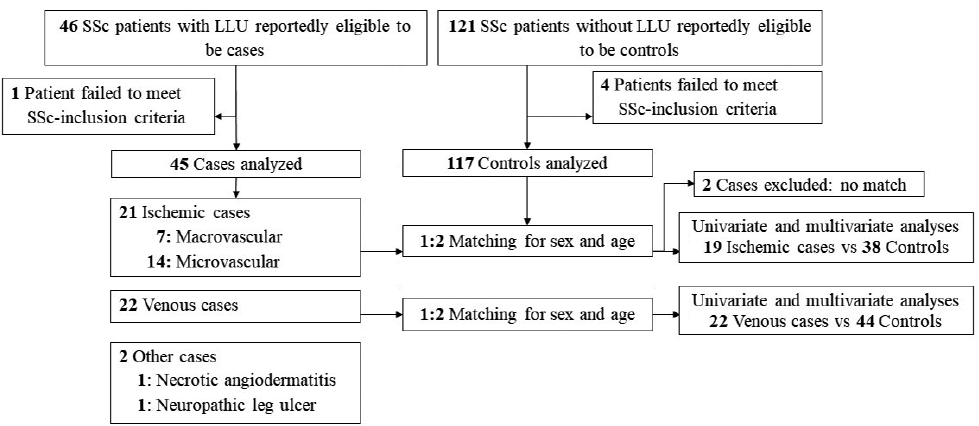
Charts of SSc patients with LLU between January 2008 and December 2013 were retrospectively reviewed by physicians in 8 French dermatology or vascular medicine departments participating in the Angio-Dermatology Group of the French Society for Dermatology to identify cases. Inclusion criteria for cases were (i) the 2013 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for SSc (12) and (ii) at least one wound below the knee lasting more than 3 months (LLU). Patients with hyperkeratosis and/or calcinosis without ulcers were not included in this study. Each SSc and LLU diagnosis was centrally reassessed by 2 study investigators to ensure that it satisfied these criteria (Fig. 1). SSc onset was defined as the date when symptoms met the ACR criteria. Patients with LLU reported the date of LLU onset at the first consultation.
Fig. 1. Flow chart for selection of cases and controls and their progression through the study. SSc: systemic sclerosis; LLU: lower-limb ulcers.
For the descriptive analysis of cases, LLUs were classified as venous, arterial macrovascular, microvascular or other aetiology LLU, according to the following parameters: (i) LLU of predominant venous cause were defined by: clinical findings consistent with established venous disease (skin hyperpigmentation, varicose veins, lipodermatosclerosis) and confirmation by venous duplex ultrasonography (US). Patients with mixed LLU (i.e. with both arterial and venous diseases) were classified as venous LLU in cases of non-significant arterial stenosis; (ii) LLU of predominant arterial macrovascular cause was defined by clinical findings consistent with peripheral arterial disease of the involved limb (intermittent claudication, rest pain or ankle-brachial pressure index (ABPI) < 0.7) and the presence of significant (> 50%) arterial stenosis in Doppler US and/or arteriography; (iii) LLU of microvascular origin was determined after excluding other causes, as already described in the literature (11, 13): arterial macrovascular and venous causes were excluded by US Doppler; mechanical causes (traumatic or hyperkeratosis) were excluded by medical history; other causes were excluded by medical examination, with cutaneous biopsy if necessary (i.e. palpable or necrotic purpura) and electromyogram in cases of peripheral neuropathy symptoms; (iv) LLU related to other aetiologies (pyoderma gangrenosum, vasculitis, cancer) was defined by suggesting clinical findings with pathological confirmation.
As the previous literature suggested a high morbidity in ischaemic LLU patients (8–10), we looked for SSc characteristics associated with ischaemic LLU among our cases. We therefore compared cases with ischaemic LLU to controls. The control population comprised all consecutive SSc patients without any prior history of LLU recruited between January 2008 and December 2013 in the referral dermatology department of Tenon Hospital (AP-HP, Paris, France) (Fig. 1). This centre was chosen for control recruitment to estimate the LLU prevalence in SSc patients because the SSc-patient cohort from that centre was shown to be comparable to other such cohorts previously reported (14). The identification of cases and controls in this centre was performed by a database search on the terms “sclerosis”, “systemic sclerosis” and “ulcer”. The entire medical file of each case was reviewed and controls’ SSc diagnoses were verified to ensure that patients satisfied the ACR/EULAR classification criteria.
The following information from case and control patients was collected using a standardized anonymous report form after complete examination of patients’ medical charts: demographics, medical history, cardiovascular risk factors (hypertension, diabetes, dys-lipidaemia, former or current smoker, and obesity defined by a body mass index > 30); the following SSc characteristics were also collected: age at diagnosis, disease duration, subtype (diffuse, limited or sine scleroderma), cutaneous sclerosis localizations, history of cutaneous calcinosis, Raynaud’s phenomenon, prior DUs, nailfold capillaroscopy data, serologic results (antinuclear, anti-centromere, anti-topoisomerase-I antibodies, lupus anticoagulant), and visceral involvement: echocardiography-assessed heart disease (left ventricular ejection fraction < 60%), lung involvement (diagnosed using thoracic high-resolution computed-tomography scan and pulmonary function tests) and pulmonary arterial hypertension, defined as echocardiography-estimated systolic pulmonary pressure > 30 mmHg or right heart catheterization-measured mean pulmonary pressure > 25 mmHg (15).
For case patients, the following LLU parameters were collected: age at diagnosis, lesion duration, clinical wound characteristics, number of wounds, pain treatment, prothrombotic factors, dosage results, vascular investigations at wound diagnosis (ABPI, toe pressure, venous and arterial Doppler US and arteriography), and clinical LLU outcome during follow-up, including time-to-healing and relapses.
Descriptive and comparative analyses were computed with StatView software (v5.0, SAS Institute Inc). Quantitative variables are expressed as medians (range) and qualitative variables as number (%). As we aimed to point out clinical factors relevant to severe prognosis, which has been shown in the literature to be related to ischaemia (9, 10), and as macrovascular LLU might also have a microvascular component (11), we pooled arterial macrovascular and microangiopathy-related LLUs into an “ischaemic LLU” group for comparative analyses that excluded the other LLU types.
Among the control population, 2 controls were matched to each case based on sex and age within 2.5 years (Fig. 1). When certain cases could be matched with more than 2 controls, a person uninvolved in the study randomly selected the 2 controls retained. Cases without a control-group match were excluded from the comparative study to avoid negatively impacting the statistical results (Fig. 1). Univariate comparisons between cases and controls used a Student’s t-tests or Mann–Whitney tests, as appropriate, for quantitative variables, and Pearson’s χ2 tests or Fisher’s exact tests, as appropriate, for qualitative variables. Associated factors were identified by univariate and backward stepwise multivariate logistic-regression analyses, with their respective significance levels set at 0.20 and 0.05.
Among the 46 cases deemed eligible during the study period, one not meeting ACR/EULAR SSc criteria was excluded, leaving 45 cases in the study group (Fig. 1); among them, 15 were from the referral centre that also recruited 117 eligible controls during the study period for comparative study.
A venous cause was predominant in 22 patients (49%) and an ischaemic cause in 21 patients (47%), attributed to macrovascular involvement in 7 cases (16%) and microvascular involvement in 14 (31%). Six patients (13%) had multifactorial LLU causes: 4 macrovascular LLU-subgroup patients had past (n = 3) or present (n = 1) venous insufficiency; 2 venous LLU-subgroup patients had non-significant arterial stenosis. Two cases (4%) had LLUs of other aetiology that were caused, respectively, by peripheral neuropathy and typical necrotic angiodermatitis (16). Cases’ SSc characteristics and LLU characteristics are reported in Tables I and II and Table SI, respectively, according to LLU aetiology, except for the 2 cases with other aetiologies, which were excluded from comparative analyses and Tables.
Table I. Systemic sclerosis (SSc) characteristics of the cases
Table II. Characteristics and outcomes of systemic sclerosis (SSc) patients’ lower-limb ulcers (LLUs)
The first LLU episode occurred a mean of 10.3 years after SSc diagnosis for 40 of the 45 patients, and a mean of 4.8 (range, 0.7–11.8) years before SSc diagnosis for the remaining 5, whose LLUs were caused by venous insufficiency. In 19 cases (42%), patients had experienced at least one LLU before study inclusion and all those LLUs shared the same aetiology as the study lesion. Venous LLUs most frequently involved the ankle, while macro- and microvascular LLUs affected the feet. Patients with macrovascular LLUs were older and had longer-lasting SSc at the time of the first LLU episode than the other LLU subgroups. Macrovascular LLUs were more frequently multiple, with longer durations than the other LLUs. Only LLUs of ischaemic origin related to macro- and/or microvascular involvement required amputation (28.6%). Among all causes, macrovascular LLUs had the poorest outcomes with the highest amputation rate (4 of 7 cases, 57%), lowest healing rate (57%), longest mean time-to-healing (16.0 months) and highest relapse rate among those whose LLU had healed (75%). In macrovascular LLUs, all 4 amputations were made necessary by disease progression despite vasodilator drugs, and despite arterial revascularization in 3 cases. Three patients relapsed within 6 months post-amputation. In the microvascular subgroup, neither of the 2 amputees relapsed during follow-up.
The percentage of cases receiving immunosuppressive drugs that might have impaired healing function were similar for the 3 aetiologic subgroups (29% for macrovascular, 36% for microvascular and 29% for venous LLUs). The durations of LLU follow-up for cases with complete healing or not and between the 3 different aetiologic subgroups did not differ significantly.
In the referral centre where the control population was recruited, the estimated LLU prevalence reached 12.8% of SSc patients (15 cases and 117 controls during the study period). Sex and age matching of each ischaemic LLU case (n = 21) with 2 controls was possible in all cases except 2 with microvascular LLUs, where no correspondence for age could be found in the control group. These 2 cases were excluded from the comparative analyses, which therefore included 19 cases of ischaemic LLUs and 38 matched controls, selected randomly among eligible controls (Table III). The clinical factors significantly associated with ischaemic LLUs (p < 0.05) were at least 2 cardiovascular risk factors, longer duration of SSc follow-up, sclerosis involvement of the feet or legs, previous or concomitant DUs, cutaneous calcifications, pulmonary arterial hypertension, pulmonary fibrosis and anti-topoisomerase-I antibody-positivity (Table III).
Table III. Univariate analysis: systemic sclerosis (SSc) patients’ factors associated with ischaemic lower-limb ulcers (LLUs)
Regarding venous LLU, 22 cases were compared to 44 randomly selected controls. Clinical factors associated significantly with venous LLUs were a history of cutaneous calcifications, a history of deep venous thrombosis, the presence of a pulmonary arterial hypertension and the presence of pulmonary fibrosis (Table SII).
During follow-up, 2 cases died of infections; one each from the microvascular and macrovascular LLU subgroup, respectively at ages 93 and 77. No controls died.
Because the variables “sclerosis localized in the feet” and “in the leg” were statistically associated, only the first was kept for multivariate analysis. Logistic-regression multivariate analyses retained past/concomitant DU (odds ratio [OR], 21.42; [95% CI 1.94–236.99]; p = 0.0125) and the sclerosis localization in the feet (OR 34.52; [95% CI 5.25–227.01]; p = 0.0002) as independent risk factors for ischaemic LLUs. For this logistic-regression model, R2 was 0.550; 84.2% of SSc patients with ischaemic LLUs had past/concomitant DUs and foot skin sclerosis, while no controls had these 2 manifestations.
For venous LLUs, logistic-regression multivariate analyses retained a history of cutaneous calcinosis (OR, 4.53; [95% CI 1.22–13.42]; p = 0.0220) and pulmonary arterial hypertension (OR 16.98; [95% CI 1.77–161.92]; p = 0.0140) as independent risk factors. Nevertheless, for this logistic-regression model, R2 was low (0.175), limiting the value of these results.
Our results showed that LLUs occurring in SSc patients may be caused by predominant venous insufficiency (49%) or ischaemia (47%) related to macrovascular and/or microvascular involvement. The latter seems to be more frequent in SSc patients than the general population for whom predominant arterial LLUs account for 20–40% of chronic wounds (17, 18). SSc LLUs healed poorly, especially ischaemic macrovascular LLUs, which have a 57% amputation rate, long mean time-to-healing (16.0 months) and a 75% relapse rate. In our study, ischaemic LLUs were independently associated with past/concomitant DUs (OR: 21.4) and foot skin sclerosis (OR: 34.5).
One limitation of this study is its retrospective design and the recruitment of matched controls in a dermatology department, indicating a 12.8% LLU frequency in SSc patients. Another is the difficulty of classifying LLUs in SSc, notably microvascular LLUs that are defined in this study, as in previous ones, by the exclusion of other causes, without systematic assessment of toe pressure measurement (11).
In this large multicentre study focusing on LLU in SSc patients, the most frequent LLU aetiology was venous insufficiency (49%); mixed arterial and venous aetiology accounted for 13% of cases, which is similar to what has already been reported in the literature (9, 11, 19).
In recent decades, macrovascular disease involving lower-limb arteries in SSc patients has been highlighted in several small series (10, 20, 21). Microangiopathic LLUs and LLUs associated with peripheral macrovascular involvement have also previously been reported as case reports or short series (8, 11, 22–25). Arterial macrovascular involvement in SSc may be secondary to multiple factors such as endothelial dysfunction, chronic inflammation, disease duration, and traditional cardiovascular risk factors (26–31). In our study, ischaemic macrovascular LLUs with significant arterial involvement in arteriography accounted for 15% of LLUs, close to the 10.8% reported by Blagojevic et al. and to the 10% to 20% of SSc patients reported as having symptomatic lower-limb peripheral arterial disease (11, 28, 32, 33). Ischaemic macrovascular LLUs were observed in patients without traditional cardiovascular risk factors, in agreement with previous studies (11, 29).
Microvascular disease was the second most frequent LLU aetiology in our study (31%). This finding supported that microvascular disease is a common feature of SSc, which may also affect the lower limbs, with endothelial dysfunction in capillaries and arterioles engendering disturbed vasomotor regulation and structural changes as with DUs.
The rarity of other aetiologies in our study (neuropathy and necrotic angiodermatitis) also agrees with the literature, where miscellaneous causes were reported for 10% of LLU patients (34).
All LLU subgroups had poor outcomes; these were particularly dire for the macrovascular subgroup, where amputation was required for 28.6% of SSc patients with ischaemic LLUs, versus 0% for other causes. Little information is available in the literature on SSc patients’ LLU outcomes: Reidy et al. (23) reported 7 amputations in a cohort of 1,030 SSc patients; Youssef et al. (21) had 5 major amputations in a series of 31 SSc patients, among whom 58% had peripheral arterial disease; Hafner et al. (9) described 3 patients whose arterial revascularizations allowed complete healing. In our series, ischaemic LLUs healed poorly despite optimal medical treatment and arterial revascularization, leading to amputations in 4 of the 7 patients with macrovascular LLUs and 2 of the 14 patients with microvascular LLUs. Despite our low number of SSc patients with macrovascular LLUs, the 57% amputation rate and 75% relapse rate were higher than those reported for non-SSc patients with peripheral arterial disease and concurred with case reports of SSc-related LLUs (10, 35).
In the venous subgroup, nearly 60% of patients’ LLUs healed, as commonly reported for venous LLUs in non-SSc patients, but their 69% relapse rate was unusually high compared to non-SSc patients (36).
Our multivariate analyses retained ischaemic LLUs as being significantly associated with past/concomitant DUs (OR, 21.42) and sclerosis involving the feet (OR, 34.52). These associations are logical because cutaneous sclerosis severity reflects microvascular impairment due to SSc, which may cause DUs. They were not found by Blagojevic et al. (11) when comparing SSc patients with “pure microvascular ulcers” to SSc patients with lower-limb, non-ulcerated lesions (i.e. calcinosis and hyperkeratosis). It is difficult to rule out that patients with significant arterial stenoses, and who were therefore classified as having macrovascular LLUs, did not have microangiopathy involvement as well. This prompted us to pool macrovascular and microvascular LLUs in an ischaemic group, considering that they shared common clinical pattern and prognosis.
Some other factors significantly associated with ischaemic LLUs in univariate analyses, e.g. anti-topoisomerase-I antibody-positivity, diffuse SSc subset and SSc duration, which were also associated with DU occurrence in the literature (37, 38) failed to reach significance in our multivariate analyses, probably because of a lack of study power. Because of the retrospective setting of the study, we only recorded the history of calcinosis rather than a concomitant calcinosis at inclusion date. This is a limitation of our study that poorly estimated calcinosis frequency.
In conclusion, our results showed that LLUs in SSc patients are not infrequent and may be related to venous disease, but also, in half of cases, to microcirculation impairment and/or severe lower-limb macrovascular involvement. SSc patients’ LLUs had particularly poor outcomes when the cause was ischaemic with micro- or macrovascular involvement, with high amputation and relapse rates. Ischaemic LLUs in SSc were significantly associated with past/concomitant DUs and cutaneous sclerosis of the feet or legs, rather than with usual cardiovascular risk factors. The strength of these associations led us to consider systematic lower-limb arterial screening during follow-up of SSc patients with those 2 symptoms, especially because SSc patients are mostly young women for whom this screening is not usual.
We thank Pr Eric Vicaut and Dr François Chasset for providing a critical review of the manuscript. The authors thank Janet Jacobson and Andrew Cowderoi for English editing of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize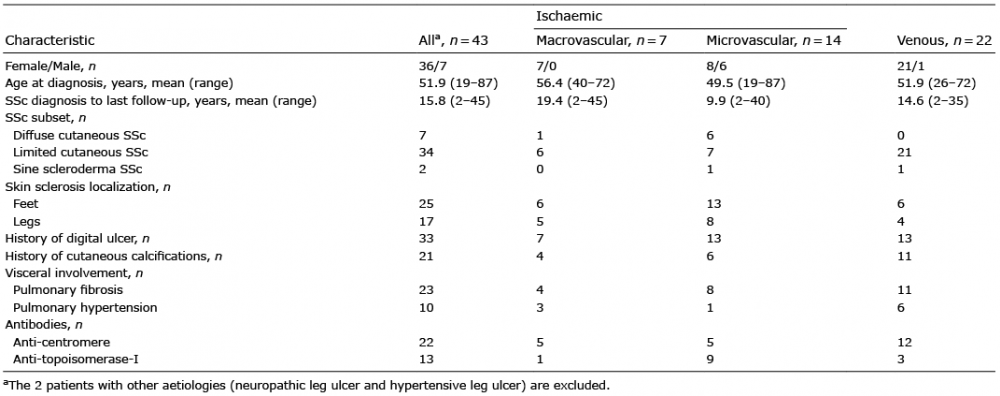 Click to show fullsize
Click to show fullsize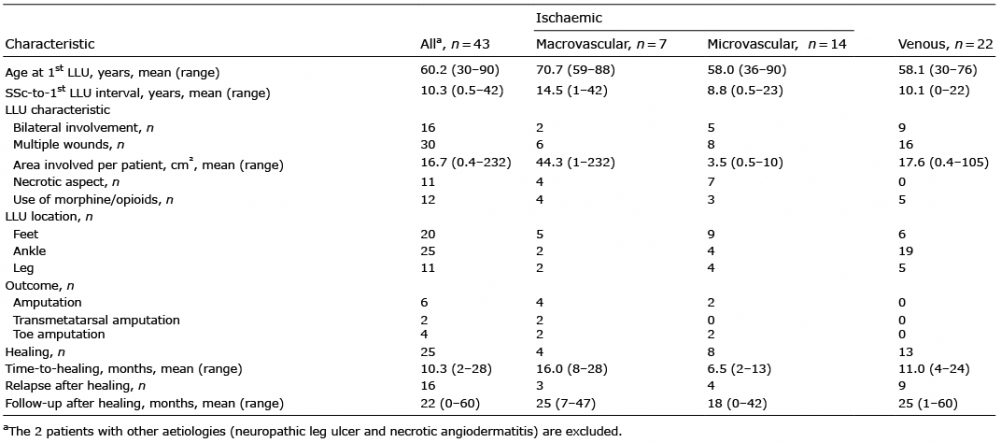 Click to show fullsize
Click to show fullsize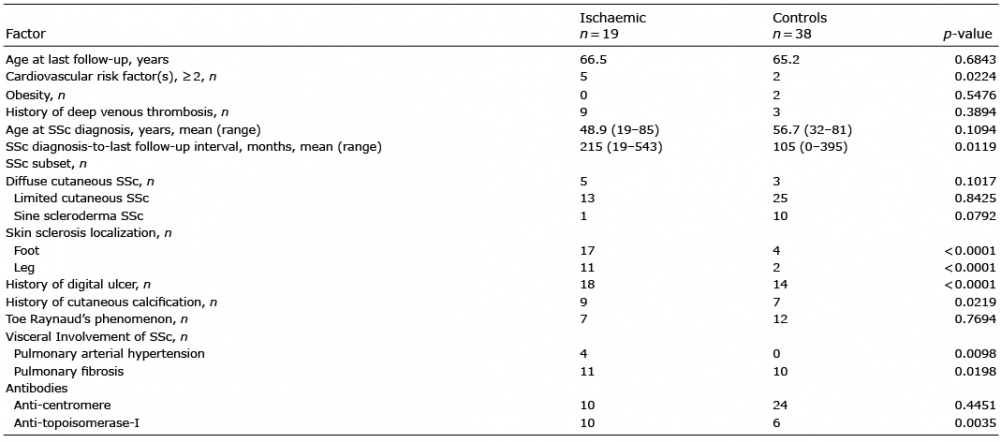 Click to show fullsize
Click to show fullsize